
Office syndrome is the everyday name many desk workers use for the pattern of neck stiffness, shoulder fatigue, jaw tension, eye strain and recurring headaches that can build up after long hours at a screen. It is not a single medical diagnosis. It is a useful training concept because it reminds therapists to look at the whole workstation body: upper cervical joints, suboccipital muscles, pericranial tenderness, breathing, jaw clenching, visual load and stress physiology. For students at Nuad Thai School, this article turns that broad idea into a careful manual therapy map.
The focus here is cervicogenic headache and tension-type headache, two patterns that often appear in office clients but should never be casually merged. A cervicogenic pattern suggests that the neck is a meaningful driver of head pain, often with reduced cervical range, posterior-to-anterior pain referral or provocation from neck movement. A tension-type pattern is usually described as pressing or tightening, often bilateral, mild to moderate, and commonly associated with pericranial tenderness. The overlap is real, but the therapist's duty is to observe, adapt and refer when symptoms step outside the wellness scope.
This guide is educational, not diagnostic. Massage and manual therapy may support comfort, relaxation, tissue awareness and mobility for some people, but they do not replace medical assessment. New severe headache, neurological signs, fever, trauma, sudden onset, visual loss, unexplained vomiting, cancer history, immune suppression, pregnancy-related warning signs or headache that is changing rapidly should be referred to a qualified health professional before spa-based treatment.
Key Takeaways
- Office syndrome headaches often involve a loop between neck posture, suboccipital guarding, jaw tension, visual strain, stress and reduced movement variability.
- Cervicogenic headache is not simply 'tight neck equals headache'; it requires cautious reasoning about neck-related causation and symptom behavior.
- Tension-type headache has a strong neurobiological component, especially when it becomes frequent or chronic; pressure should be calming and graded, not aggressive.
- The suboccipital area matters because upper cervical input can converge with trigeminal sensory pathways, helping explain pain felt around the head, temples or eyes.
- TMJ and eye-strain questions belong in an office-syndrome intake because jaw clenching and visual fatigue can maintain head, face and neck discomfort.
- A safe protocol combines screening, gentle assessment, suboccipital and cervical soft-tissue work, shoulder-girdle release, jaw-aware cues, eye-rest education and home-care advice.
Training Infographic
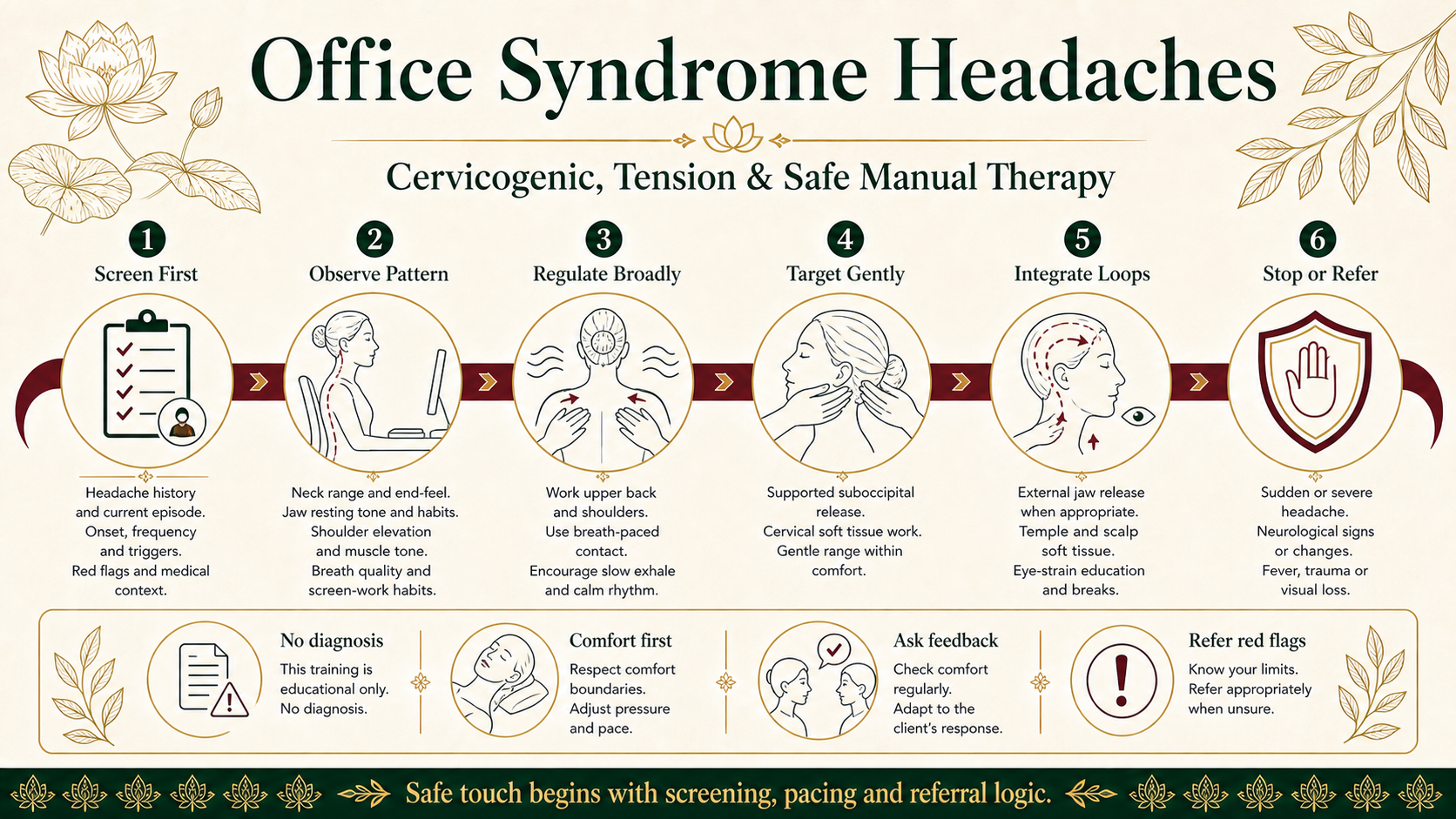
What Office Syndrome Means in a Headache Article
In a spa or massage school context, office syndrome usually describes the repeated stress pattern of modern desk life. The head is held forward to read the screen, the shoulders rise slightly during concentration, the thoracic spine rounds, the jaw closes harder during deadlines, breathing becomes shallow and the eyes keep focusing at a fixed near distance. None of these small events is dramatic alone. The problem is repetition. When the nervous system receives the same postural and visual signals for hours, muscles that should alternate between activity and rest may stay mildly contracted.
A therapist should not reduce this to bad posture. Many office workers use the posture they need to survive the task in front of them. The better question is whether the body has enough options. Can the person rotate the neck without fear? Can the upper ribs move when they breathe? Can the jaw rest with the tongue relaxed? Can the eyes look away from the screen often enough? Manual therapy works best when it gives the client more comfortable options rather than scolding them into a rigid ideal.
Cervicogenic Headache vs Tension-Type Headache
A cervicogenic headache is classically understood as head pain caused by a disorder of the cervical spine or its soft tissues. The International Classification of Headache Disorders notes features that may point toward this pattern: reduced cervical range of motion, worsening with provocative neck movement, side-locked pain, reproduction by pressure on neck muscles and pain that travels from the back of the head toward the front. These signs are useful, but they are not absolute proof. Imaging changes in the neck can appear in people without headaches, and neck tenderness can also occur with migraine or tension-type headache.
Tension-type headache is usually described differently. It is commonly bilateral, pressing or tightening rather than pulsating, mild to moderate in intensity and not usually worsened by ordinary activity such as walking. It can be associated with pericranial tenderness, meaning tenderness in scalp, jaw, temple, neck and shoulder muscles when palpated. The modern view is not that it is imaginary or merely psychological. More frequent forms involve neurobiological mechanisms, peripheral tissue sensitivity and central pain processing. That is why heavy pressure is not automatically better.
For office syndrome clients, the distinction matters because the treatment logic changes. A clearly neck-provoked pattern asks for careful upper cervical assessment, gentle mobilizing influence through soft tissue and range, and attention to the shoulder girdle. A tension-type pattern asks for broader regulation: calming contact, scalp and temple work, jaw awareness, breathing, ergonomic pacing and pressure that reduces guarding. Many clients show mixed features, so the session should stay flexible.
Neurological Pathways of Tension Headaches
Headache pain is not only a muscle problem. Sensory information from the upper neck, cranial tissues, face and jaw is processed through networks that include the trigeminal system and upper cervical nerves. Clinicians often discuss the trigeminocervical complex when explaining why a problem in the upper neck can be felt in the head, and why head pain can be accompanied by neck sensitivity. This does not mean every tight neck causes a headache. It means the map is shared enough that therapists must think in systems.
In tension-type headache, peripheral tenderness can feed the system, especially from pericranial muscles such as temporalis, masseter, sternocleidomastoid, trapezius and suboccipitals. If the headache becomes frequent, the nervous system may become more responsive to normal input. A client may then feel tenderness from pressure that would not bother another person. This is one reason the Nuad Thai School approach emphasizes dosage. The therapist should start with broad, slow, predictable contact and only increase specificity when the tissue and the client both respond well.
The nervous system also listens to context. Deadlines, poor sleep, dehydration, fear of pain and long visual concentration can all change how touch is received. A technically correct stroke performed with rushed rhythm may be less helpful than a simpler technique delivered with excellent pacing and communication. For office syndrome headaches, the goal is not to overpower the pain pathway. The goal is to lower threat, improve movement confidence and help the client feel that the head, neck, jaw, eyes and shoulders can cooperate again.
Suboccipital Muscle Tension
The suboccipital muscles sit deep at the base of the skull. They help fine-tune head position and upper cervical movement. In office workers they may become guarded when the head is held slightly forward and the eyes keep making small adjustments toward a screen. Clients often describe this as a tight band at the skull base, pressure behind the eyes, or a headache that begins at the back of the head and travels upward. These descriptions are common, but the therapist should still screen for red flags and avoid promising a specific diagnosis.
Suboccipital work should be precise but gentle. The therapist can begin with the client supine, the head supported, and fingers placed under the occiput without poking. The first contact is listening: feel whether the client can let the head become heavy. Then use sustained, low-force contact, small traction-like unloading and breath-paced holds. If the client braces, holds the breath, reports sharp pain, dizziness, nausea, visual change or nerve symptoms, the technique should stop. Strong pressure into the upper neck is not a badge of skill.
A useful teaching cue is to treat the suboccipitals as a conversation with the nervous system. The tissue is deep, sensitive and close to important cervical structures. Students should keep their wrists relaxed, avoid levering the neck, and never chase a trigger point aggressively. When the area softens, reassess gentle neck rotation, jaw resting position and the client's perception of head pressure. The change should feel easier, not forced.
Eye Strain and Headache Correlation
Digital eye strain, sometimes discussed as computer vision syndrome, can include tired eyes, blurred vision, dryness, burning, difficulty refocusing, light sensitivity and headache. For massage students, this matters because eye strain does not stay in the eyes. A client who squints, leans toward the screen or keeps the brows lifted may recruit forehead, temple, jaw and neck muscles all day. The neck then receives the blame even though the visual system helped create the load.
The intake should ask simple questions: How many hours do you use a screen? Do headaches increase late in the workday? Do you wear the correct prescription? Is the monitor too high, low, bright or close? Do you get dry eyes? Do you notice brow tension or jaw clenching when reading? These questions do not turn the therapist into an eye doctor. They identify whether massage should be paired with practical advice: screen breaks, distance changes, lighting adjustments and referral for vision assessment when symptoms are persistent.
Manual therapy can support the surrounding pattern with gentle work around the temples, forehead, scalp, jaw, neck and shoulders. Avoid direct pressure on the eyeball. Avoid claiming that massage corrects vision. A clean professional message is stronger: if visual load is contributing to headache, local soft-tissue work may feel good, but the visual habit also needs to change.
TMJ Involvement in Office Syndrome
The temporomandibular joint and chewing muscles are often part of the office syndrome picture. Many clients clench during concentration, hold the teeth lightly together while typing, chew gum during stress or sleep poorly with jaw tension. The masseter and temporalis are not isolated from headache patterns. They share sensory relationships with the trigeminal system, and temporomandibular disorders are commonly discussed alongside headache conditions.
A massage therapist should use jaw-aware screening without overstepping. Ask whether the client has jaw clicking, locking, pain when chewing, morning jaw fatigue, dental splints, recent dental work or known TMJ diagnosis. If there is locking, severe pain, trauma, bite change or dental concern, refer. If the issue appears to be ordinary clenching tension, external work on masseter, temporalis, scalp and neck may be appropriate within training and local scope. Intra-oral techniques require specific training, consent and legal permission; they should not be improvised.
A simple home cue can be powerful: lips together, teeth apart, tongue resting gently on the palate, slow nasal breath. This does not treat a disorder, but it teaches the client to notice unnecessary jaw effort. During the massage session, students should check whether suboccipital release changes jaw resting tone and whether gentle jaw softening changes the neck. Office syndrome is full of these loops.
Manual Therapy Protocols for Office Syndrome Headaches
A professional protocol begins before touch. The therapist screens for red flags, clarifies headache behavior, asks about medical diagnosis and medication, and identifies what makes symptoms better or worse. Important questions include: Is this headache new or familiar? Was onset sudden? Is there fever, trauma, neurological change, fainting, cancer history, pregnancy concern or visual loss? Does coughing or exertion make it worse? Is pain side-locked, bilateral, behind the eyes, in the temples or at the skull base? How often does it happen?
The second step is observation. Look at how the client sits, turns the head, breathes, opens the jaw and rests the shoulders. Do not turn this into criticism. Observation guides dosage. A client with high irritability, light sensitivity or chronic daily headache may need a shorter, quieter session. A client with simple workday stiffness may tolerate broader shoulder, upper back and neck work before specific suboccipital contact.
The third step is broad regulation. Begin with slow contact through the upper back, shoulders and chest wall. Work on trapezius, levator scapulae, cervical paraspinals and upper thoracic fascia with comfortable pressure. Add gentle shoulder mobilization and breath cues. This prepares the nervous system before precise neck work. For Thai massage students, body mechanics are essential: use body weight, stable stance and calm rhythm instead of thumb strength.
The fourth step is targeted cervical and suboccipital work. Use supported positioning. Apply gentle sustained holds under the occiput, soft tissue spreading along the cervical paraspinals and careful work around sternocleidomastoid and scalenes without compressing the front of the neck. The aim is not to erase every tender point. The aim is to reduce guarding and improve the client's sense of ease. Reassess range and symptoms after each small section.
The fifth step is jaw, scalp and eye-strain integration. External masseter and temporalis work can be included when appropriate. Scalp work can be slow and grounding. Around the eyes, keep pressure on the brow, forehead and temples, never on the eye itself. Teach microbreaks: look away from the screen, breathe into the ribs, release the teeth, lower the shoulders and move the neck gently. These small behaviors extend the session into daily life.
The final step is aftercare and referral logic. Recommend hydration, sleep attention, screen pacing, gentle movement and professional evaluation when symptoms are unusual or persistent. A therapist can say: 'Today your neck and jaw tension seemed connected with your headache pattern, and the work reduced some sensitivity. Because headaches have many causes, please seek medical advice if the pattern changes or if warning signs appear.' That sentence is humble, safe and professional.
Protocol Matrix for Students
| Stage | What to Do | Why It Matters | Stop or Refer If |
|---|---|---|---|
| Screen | Ask headache history, onset, red flags, medical diagnosis and medication context. | Separates wellness care from possible medical need. | Sudden severe headache, neurological symptoms, fever, trauma, visual loss or rapidly changing pattern. |
| Observe | Check neck range, jaw resting tone, shoulder elevation, breath and screen-work habits. | Shows the load pattern without blaming posture. | Movement causes sharp, unusual or spreading symptoms. |
| Regulate | Start broad: upper back, shoulders, breath-paced contact and calming rhythm. | Lowers guarding before specific neck work. | Client becomes dizzy, nauseous, anxious or more painful. |
| Target | Use gentle suboccipital release, cervical soft-tissue work and supported range. | Addresses upper cervical contribution without forcing structures. | Neurological symptoms, strong pain, visual change or intolerance. |
| Integrate | Add external jaw, temple, scalp and eye-strain education when indicated. | Connects TMJ and visual load to the office pattern. | Jaw locking, dental trauma, severe TMJ pain or eye symptoms requiring care. |
| Aftercare | Give microbreaks, gentle mobility and referral advice. | Makes the session useful beyond the massage table. | Headaches remain severe, frequent or unexplained. |
How This Fits Nuad Thai School Training
The Office Syndrome Massage Course is the natural practical path for this topic. Students learn how to organize a session around real desk-worker complaints while staying inside professional boundaries. The article gives the anatomy and reasoning; supervised training gives hand placement, pressure control, client communication and correction.
This topic also connects with Head Spa Massage, Indian Head Therapy, Private Thai Massage and Sport Massage. A strong therapist does not memorize a single headache routine. They learn to choose from a menu: calming scalp work, neck and shoulder release, thoracic mobility, jaw-aware work, breath regulation and practical self-care advice.
Frequently Asked Questions
Can massage cure cervicogenic or tension headaches?
No. Massage should not be presented as a cure. Manual therapy may support comfort, relaxation, mobility and body awareness for some clients. Diagnosis and medical treatment belong to qualified healthcare professionals.
Why do office headaches often start at the base of the skull?
The upper neck and suboccipital region help control head position. Prolonged screen work can increase guarding there, and upper cervical sensory input can relate to head pain pathways. That makes the area important, but it still requires gentle work and careful screening.
Should a therapist work inside the mouth for TMJ tension?
Only with specific training, clear consent and legal permission. Many spa and massage sessions can stay external: masseter, temporalis, scalp, neck and relaxation cues. Jaw locking, bite changes, dental issues or severe TMJ pain should be referred.
What home advice is safest for office syndrome headaches?
Keep it simple: regular screen breaks, gentle neck movement, relaxed jaw position, lower shoulders, easy breathing, hydration, sleep attention and medical evaluation for unusual symptoms. Avoid extreme self-massage tools on the upper neck.
Sources and Research Notes
References used for this educational guide
- ICHD-3: Cervicogenic headache
- ICHD-3: Frequent episodic tension-type headache
- ICHD-3: Headache attributed to temporomandibular disorder
- Clinical reasoning for manual therapy management of tension type and cervicogenic headache
- Systematic review: manual and exercise therapy for cervicogenic headache
- Systematic review: temporomandibular disorders in migraine and tension-type headache patients
- Computer vision syndrome review